The importance of partnership agreements
43 In an earlier report (Ref. 9), we expressed concern about the risks that stem from inadequate protocols governing partnerships:
'…the absence of formal partnership arrangements both inhibits the achievement of the partnership's objectives and increases the potential for a breakdown in governance arrangements and controls.'
That report summarised the main findings of our auditors' work on the accounts of local authorities, NHS bodies and probation boards. We found that a substantial minority of public bodies have experienced problems with partnerships (Figure 3).
Figure 3 In 2003/04, almost all local authorities were working in partnership and a quarter experienced problems. |
|
Source: Audit Commission 2004 |
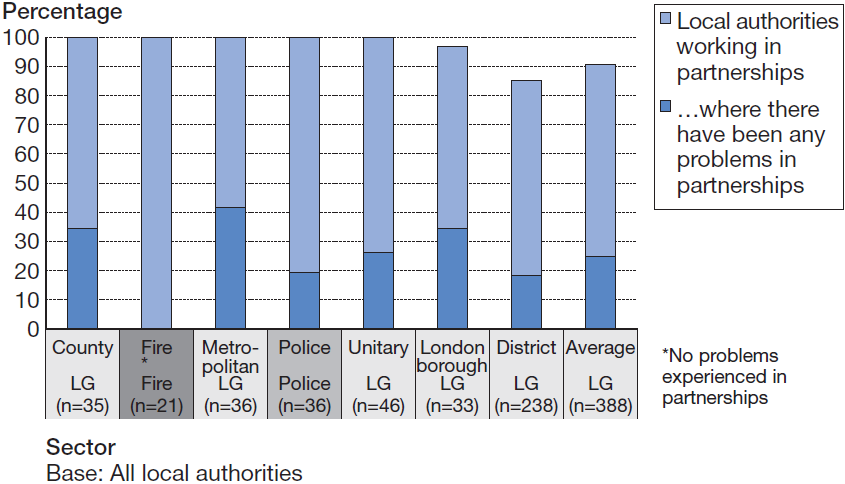
44 In the 94 authorities where we identified problems, around two in five (39 per cent) could be described broadly as facing risks relating to the absence of, or poor operation of, financial controls and governance processes in the council or one or more of its partners. Even where councils have partnership agreements, they do not always apply them uniformly to all their partnerships: only a quarter (27 per cent) of councils do so.
Box A |
The common themes that emerge from our reviews are neatly exemplified by the recommendations provided to one metropolitan district council. The audit report wanted the council to have: • a shared understanding of the roles, responsibilities and accountabilities of each partner; • a shared ownership of strategy; • better financial management, with clear procedures for determining the financial liabilities of each partner; • performance management arrangements between individual organisations and the partnership; • more structured and comprehensive reporting on performance and finance; and • evidence of the value for money of the partnership arrangements. |
Source: Audit Commission |
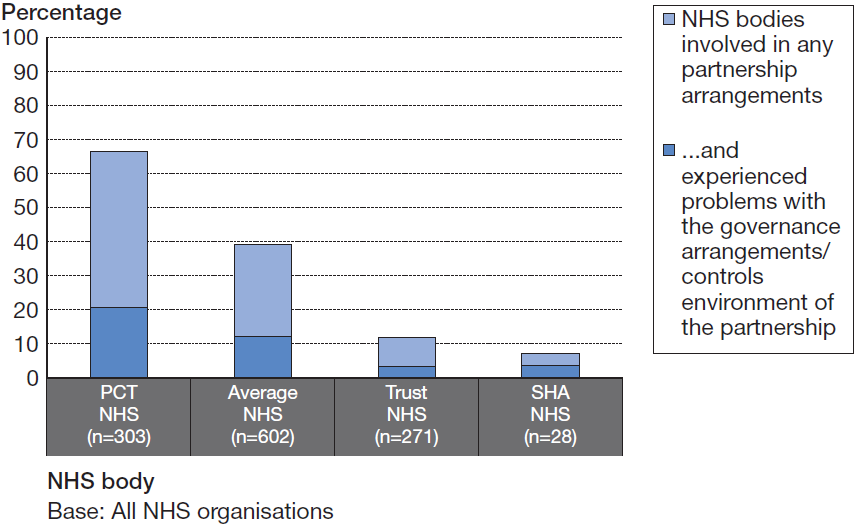
45 At the time these auditor returns were completed, a smaller proportion of NHS bodies were working in partnershipI. In 2003/04, around two in five (39 per cent) NHS bodies were involved in partnership arrangements using Health Act flexibilities. There was significant variation across the bodies: two-thirds (66 per cent) of PCTs were involved in partnerships, compared with only 12 per cent of NHS acute trusts. Two SHAs were also involved in flexible arrangements. About a third of the PCTs involved in partnerships had experienced problems (Figure 4).
Figure 4 NHS organisations also experienced problems with the governance arrangements in partnerships. |
|
Source: Audit Commission 2004 |
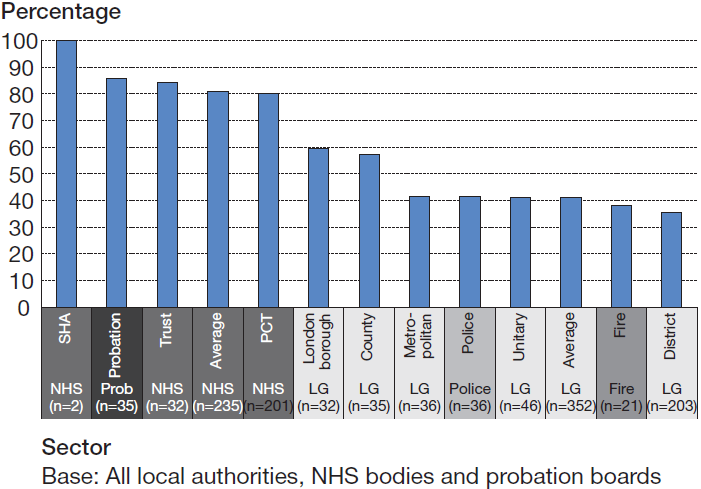
46 Despite the problems that public organisations can experience in partnership working, only two in five of all fire organisations (38 per cent), police authorities and councils (41 per cent each) involved in partnerships have partnership agreements (Figure 5). Because proportionately more NHS bodies enter partnerships using Health Act flexibilities, they are more likely to have these agreements, which set out the nature and scope of the partnership, the key risks and accountabilities. We return to this topic in Chapter 5.
47 An analysis of auditors' returns shows that PCTs without an agreement are nearly twice as likely as those with one to have problems with their partnership governance arrangements (45 per cent compared with 27 per cent). For acute trusts, the difference is even more marked - those without an agreement are nearly three times as likely to experience governance problems (60 per cent with no agreement, against 22 per cent with an agreement).
Figure 5 Proportionately more NHS organisations than local authorities have developed comprehensive partnership agreements. |
|
Source: Audit Commission 2004 |
___________________________________________________________________________
I The term partnership in this context refers to joint arrangements for health and social care using the flexibilities provided under Section 31 of the 1999 Health Act. All PCTs are statutorily involved in crime and disorder reduction partnerships and most are involved in LSPs.