The implementation was well managed
1.13 Partnerships for Health, in consultation with the Department and Partnerships UK, worked closely with the 42 local project boards. Each was assigned a facilitator from Partnerships for Health to aid in setting up the LIFTCo. We surveyed project directors across the 42 schemes and identified that 88 per cent of respondents rated the facilitators as a moderately or highly useful resource. There has been no central assessment of the performance of these individuals although Partnerships for Health obtained informal feedback from local LIFT project directors. Regular liaison between senior management from Partnerships for Health and each project board ensured that local problems were identified and resolved. In particular Partnerships for Health's Chief Executive met with project teams once negotiations were well advanced to ensure that all key issues were finalised in advance of closing deals on the initial sample.
1.14 In recognition that LIFT was a new form of procurement, Partnerships for Health ensured that both the public and private sectors had opportunities to learn about the initiative. Sources of information for prospective participants in LIFT included conferences, a dedicated website and individual meetings with senior Partnerships for Health representatives. We surveyed all shortlisted bidders across the 42 LIFT schemes and 93 per cent of respondents felt that prior to bidding for LIFT they were able to develop their knowledge of the initiative adequately through these sources. 64 per cent of respondents also believed that the market for investment in primary care prior to LIFT was undeveloped and that Partnerships for Health were crucial in stimulating their interest. Partnerships for Health were supported in developing LIFT by external organisations with an interest in a particular aspect of the initiative. 4Ps, for example, part of the Local Government Association, advised Local Authorities on their involvement in LIFT. Additionally, the Commission for Architecture and the Built Environment (CABE) assisted a small number of schemes through their Enabling Programme (Appendix 3). CABE will also assist schemes in the planned fourth wave.
1.15 Partnerships for Health were supported by KPMG and Bevan Ashford, who were appointed as central advisors for the first wave on financial and legal matters respectively, following open competition. The advisory teams were instrumental in developing the standardized procurement process and supporting documentation and in advising the first wave of LIFT schemes. The market for providing local advice was then opened out for the second and third waves to test the competitiveness of the initial advice. The process for appointing advisory teams was robust, and advisory teams who had represented the public sector were prevented from advising first and second wave private sector bidders.
1.16 Partnerships for Health allowed advisors to the public sector on first and second wave schemes to advise third wave bidders. As some bidders have won schemes across the three waves and as all waves were being developed simultaneously, they would be able to advise third wave private sector bidders what returns and concessions had been agreed in a range of earlier deals. Partnerships for Health think that such information was readily available and, in any case, they valued transfer of ideas between the public and private sectors. We agree that these arguments have some force, particularly in a mature market. LIFT was, however, still a new initiative when the third wave was announced in August 2002.
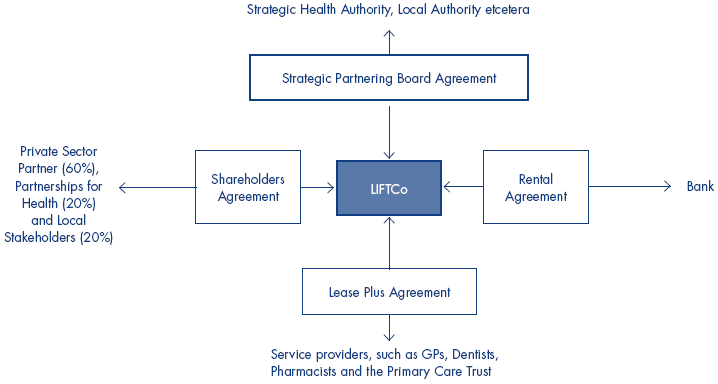
1.17 Partnerships for Health developed a suite of guidance notes and standardised contract documentation (Figure 4 overleaf) for all schemes, using their experience of PFI as a starting point. The time spent on developing the standard contracts was longer than anticipated at the outset, and several versions were issued before finalized documents were agreed. The standard documentation was often amended following local negotiations. Nevertheless, its existence resulted in time and money savings in setting up LIFTCos and getting projects underway. We questioned whether there were benefits in extending standardization beyond these traditional parameters. Partnerships for Health are understandably reluctant to impose standard buildings on diverse local areas, but recognise there may be additional untapped benefits in using standard modular designs for rooms within the LIFT building. We note there may also be potential to standardise the interior configuration of buildings with a view to enhancing the "patient journey". One area visited analysed the usage of different primary care services and had designed the flow of rooms in their building to reflect this research.
4 | Primary standard agreements between LIFT participants |
Source: National Audit Office | |